Adult Brachial Plexus Injury
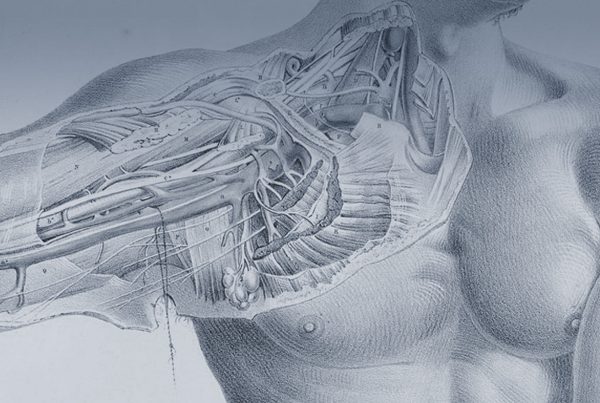
The brachial plexus is a collection of interconnected nerves in the neck and shoulder that control the arm and hand. It is an area of very concentrated function, an injury to this structure can have huge impact upon function creating in an inability to move the arm, numbness, tingling and pain (there are also effects on the skin, sweating and hair growth).
The Brachial plexus can be injured in a huge variety of ways – blunt trauma is the most common in the UK but we also see penetrating trauma such as stabbings and ballistic injuries too (bullet and gunshot wounds). Of the Blunt trauma injuries we classify these according to the ‘mechanism of injury’ this means the way that the injury happened and the amount of force that was involved. As you can imagine the injury from crashing a motorbike at 100mph is very different to slipping on a wet floor. We also use an assessment of which part of the brachial plexus has been injured – with the collar bone (clavicle) being the boundary between the nerves above it – supraclavicular injuries and those below – infraclavicular injuries.This method of classification also has cross over with the mechanism classification as supraclavicular inuries only really occur in high energy accidents where as the more vulnerable infraclavicular plexus can be inured more readily and can occur with sometime innocuous injuries.
Suparaclavicular Brachial Plexus injuries
As we have said before these injuries are most commonly caused by motor vehicle accidents especially motor bike crashes. The injury is most commonly a forced movement of the head towards on side of the body. The opposite side of the neck sustains a stretch injury and this injures the nerves.
Avulsion
The most severe of these injuries is an Avulsion. This is where the peripheral nerve root is pulled clean out of the spine. It is really a spinal cord injury and is impossible to cure completely.
The only way to improve the situation here is to try to redirect part of a nerve which are not avulsed to grow into the damaged nerve. There is a situation where all five of the nerve roots of the brachial plexus are avulsed and this is called a total plexus avulsion, It often occurs with damage to the nerves to the pupil and eye lid which cause a small pupil and a drooping eyelid (called a Horner’s syndrome). This is the most severe of injuries and in terms of function is catastrophic. There is a procedure which can be used in this condition (if referral is made early enough) where two or three of the nerves can be ‘reimplanted’. We are the only team in the UK (and indeed in the world) which carry out this procedure. Professor Thomas Carlstedt who was one of our colleagues until his retirement in 2013 was the person who showed that this was possible and useful.
Along with root reimplantation there is the possibility to perform transfer of nerves from out side the plexus and there are a number of options here, (spinal accessory nerve and intercostal nerves).
If there is only avulsion of some of the nerves then there are still some nerves roots which are connected to the brain via the spine and thus options to put nerve grafts in place. This is a method of laying new channels for these nerves to grow down and there for to renervate the damaged area.
Rupture
A rupture is a break in the nerve. The nerve cells can die from this injury but often they only die back a short distance and then try to grow back. The problem often is that there is scarring within the nerve or no track down which to grow. Thus there is no chance of improving function. We have options to improve function here. The most common is nerve grafting – where the damaged part of the nerve is cut out and new channels laid to allow the nerves to try to regrow. This means taking a length of nerve from another part of the body (which leaves a small area of numbness) to try an regain movement or an area of more important or useful sensation.
The other method is nerve transfer which is a newer technique popularised in the past 15 years or so where by a healthy nerve is redirected to grow into a muscle (or an area of insensate skin) to take over from the damaged nerve.
Scarring
Often a major part of the damaged done to the nerve will recover without surgery to the nerves themselves and needs no surgery. There is though often scarring which has happened due to the injury and the bleeding caused by it which strangles the nerves causing a block to the conduction of the nerves stopping that nerve’s function. It is possible to release the nerves from this strangling scar and to improve their chances of recovery. This is called a neurolysis and is the first part of any nerve operation.It is sometimes all that is necessary to gain improvement in function.